Erectile Dysfunction
Erectile dysfunction (ED) – you know the term. It’s when a man can’t get – or keep – an erection hard enough for satisfying sex. Your father or grandfather might have called it impotence, if they talked about it at all.

If you can’t get an erection at all, no matter what, that’s ED. But a partial erection – one that’s not as firm as you’d like it to be – is ED too. Maybe it only happens once in a while. Or maybe it only happens in certain situations – like when you’re with someone but not when you masturbate. It’s all ED.
Understandably, men are typically concerned about ED. Your sex life is likely to suffer – or at least change quite a bit. Your sense of masculinity may be bruised. You may be worried about satisfying your partner. And what about your overall physical health?
Don’t panic! ED is actually quite common. Most men experience it at some point in their lives. And often, it’s very treatable.
The American Urological Association estimates that 30 million men have erectile dysfunction
How common is ED?
It’s the most common sex problem men discuss with their doctors. The American Urological Association (AUA) estimates that 30 million men have ED.
ED is more common if you’re older, but younger men get it, too. If you’re not as healthy as you could be, the odds you’ll be dealing with ED go up. If you have diabetes, heart disease, or kidney disease, you’re at higher risk. Psychological issues, like depression and anxiety, can play a role as well.
Why can’t I get (or keep) a strong erection?
Ideally, here’s what happens to your penis when you get aroused: smooth muscle tissue relaxes and arteries widen. Additional blood starts to flow in. This extra blood makes your erection firm. Veins temporarily close, keeping the blood inside the penis until you ejaculate or the stimulation stops. Then the veins open up again and the blood flows back into your body.
ED is often a blood flow problem. The smooth muscle tissue might not relax or the arteries don’t open enough. Or, arteries might be blocked by plaques, as is the case the atherosclerosis (hardening of the arteries), making it more difficult for blood to flow in. In some cases, veins don’t constrict enough, so blood can’t stay in the penis.
What causes ED?
There are a number of possibilities here:
Vascular disease
Vascular disease involves damage to your circulatory system – the arteries and veins which carry blood throughout your body. Remember, “hard” arteries are “clogged” with plaques that form on your artery walls. Vascular disease makes it harder for blood to flow through your blood vessels. Less blood flow typically means a softer erection.
This is a common way for vascular disease to lead to ED. Your risk for vascular disease increases as you get older. An estimated 50 to 60 percent of men over 60 have ED due to vascular disease.
You’re more likely to face vascular disease if you have:
- Diabetes
- High blood pressure (hypertension)
- High cholesterol
- A history of smoking
Diabetes
When your blood sugar is too high, it can damage nerves and blood vessels throughout your body, including those needed for a firm erection. Your penis might not “get the message” from your brain to start an erection. And if an erection does get triggered, you might not have sufficient blood flow to keep it going. Diabetes is a huge ED risk factor. About 60 percent of men with diabetes have trouble with erections.
Drugs
Lots of medications men take have sexual side effects, which can include ED. If you take blood pressure drugs, heart medications, antidepressants, tranquilizers, or sedatives, you might see some changes in your erections. Over-the-counter meds that you buy at the pharmacy can have similar effects.
If you drink alcohol or use illicit drugs, you should watch your intake. These can cause ED, too.
Kidney and liver disease can affect your hormones and your sex life
Hormone imbalances
Most men know testosterone affects sexuality. It may surprise you though that it’s pretty rare for low testosterone to cause ED or low sex drive. Still, it does happen. Check with your doctor.
Prolactin is another hormone to watch. Men with pituitary gland tumors may have too much prolactin, which in turn reduces testosterone levels.
Kidney and liver disease can also affect your hormones and your sex life.
Obesity
We all know obesity is a growing problem in the United States. Maybe you’re struggling with your weight. You’re not alone. In 2017-2018, the Centers for Disease Control and Prevention (CDC) reported that 42% of Americans were obese – in other words, they had a body mass index (BMI) of over 30. Carrying extra weight puts a lot of stress on your body. The result can be heart disease, diabetes, and yes, ED.
Neurologic conditions
Some neurologic conditions, like paraplegia and stroke, interrupt nerve impulses from the brain to the penis. In other words, the penis won’t “know” that there’s a reason to become erect. Other neurologic conditions, such as multiple sclerosis (MS), Parkinson’s disease, and Alzheimer’s disease can lead to ED, too.
Pelvic trauma, surgery, radiation therapy
If you’ve had pelvic surgery, radiation treatment for cancer, or trauma to the pelvic region or spinal cord, you might experience ED.
For example, if you have prostate cancer, you might have your prostate removed surgically. Unfortunately, the prostate is surrounded by nerves needed for erections. Surgeons do their best to keep as many nerves intact as they can (a technique called nerve-sparing). But many men still have some degree of ED afterward. The situation usually improves, but it takes time – sometimes up to 18 months.
The situation is similar if you have a radical cystectomy for bladder cancer.
Peyronie’s disease
Men with Peyronie’s disease have a noticeable curve to their erect penis due to areas of hardened scar tissue (plaques) that form just beneath the skin’s surface. Some men with Peyronie’s develop painful erections or ED.
Venous leak
Good blood flow into the penis is critical for a firm erection. But that’s only half of the story. The blood needs to stay in place to keep a strong erection. Sometimes, there’s a problem with the veins, and they can’t keep the blood in. So it leaks back into your body. The result? A softer erection, or no erection at all.
Psychological and emotional issues
Stress and anxiety can have a huge impact on our health, including our sex lives. If you’re worried about your relationship, your kids, your job, or just life in general, that might transfer to the bedroom.
Add in anxiety about ED and things can go downhill quickly. If you’re in bed with your partner and worried about your performance, it’s going to be tough to relax – and that’s a recipe for ED.

Diagnosing ED
We know. It’s tough for many men to talk with a doctor about the possibility of ED. But your doctor has heard it all. And talking with your doctor is the first step in doing something about the issue.
Your doctor will ask the usual questions about your medical history and your lifestyle. Do you smoke? How much exercise do you get? What’s your diet like? Your doctor will also need some details about your erections. How often do you have trouble getting or staying firm? Can you get an erection in some situations (like when you masturbate), but not others? How has your sex drive been? Do you have any pain?
Again, your doctor has heard it all. Men are treated for ED every day. You want your treatment to be as effective as possible, so answer the questions with as much honesty and detail as you can muster.
Lab tests will probably be part of this too. You’ll likely have blood and urine tests. They’ll want to check how your liver, kidneys, and thyroid are working. You might even have an ultrasound to check your blood flow.
How Is ED Treated?
We’ve all seen the ads for ED drugs. But pills are only one way to treat ED. Treatments can even be combined. Work with your doctor to find the best approach. Again, the more information you provide and the more questions you ask, the more effective your treatment is likely to be.
Lifestyle changes and natural treatments
Sometimes, ED can be managed by simple lifestyle changes. For example, if you have diabetes, then controlling your blood sugar may improve your erections. Or, if you’re taking a medication with sexual side effects, tweaking your prescription might help. (Never make medication changes on your own. Always check with your doctor.)
These basic changes are the first treatment options for many men:

- Quit smoking. Your doctor can help tailor a smoking cessation plan that is right for you. You’ll feel better. You’ll look better. Your wallet will thank you.
- If you use recreational drugs, stop. Your doctor can help you here, too.
- Do you drink a lot? Does someone else in your life think you should cut back? Give it a try. Or stop completely. Again, your doctor can help you.
- Exercise! It’s the closest thing there is to a wonder drug. Start exercising (or increase your current effort even modestly) and you’ll almost immediately lower your risk for health problems. Chances are you’ll feel better too. You might lose a few pounds. Maybe your pants will fit a little better. Exercise doesn’t have to be a grind to be effective. Play some basketball. Go for a bike ride. Walking is excellent exercise.
- Change your diet. Think salads, fruits, and veggies. Whole grain breads and pastas. Soy, beans, seeds, nuts, olive oil, and cold-water fish (like salmon, tuna, sardines, halibut, and mackerel). Avoid fast food, processed foods, caffeine, and sugar.You don’t have to make drastic changes all at once. Try a salad for lunch twice a week instead of drive through. Have an apple or a peach for dessert instead of that chocolate-chip cookie. Pour yourself a glass of flavored seltzer water instead of soda or fruit punch. Get a cookbook full of healthy recipes and experiment with foods you’ve never tried before. (This can be especially fun with your partner or friends.)
Sex therapy and counseling
If anxiety, depression, or another mental health issue is triggering your ED, your doctor might suggest counseling or sex therapy. Therapy can give you a chance to talk things over with a professional and learn some coping strategies. If you have a partner, you might bring them with you. Together, you can work on your communication and your relationship.

Pills
Yes, you’ve seen and heard commercials for ED drugs. In the United States, there are four oral medications used to treat ED: sildenafil (Viagra), vardenafil (Levitra), tadalafil (Levitra), and avanafil (Stendra).
They’re called phosphodiesterase type 5 inhibitors – PDE5s inhibitors for short. And while they are all used a little differently, they work in similar ways, by relaxing smooth muscle tissue in your penis. Then, enough blood can flow in for a firmer erection.
Usually, men take PDE5 inhibitors about an hour or two before sex, but you should always follow your doctor’s instructions.
PDE5 inhibitors are effective for about 70% of men, but they’re not safe for everyone. Men who take nitrates for heart conditions should never take PDE5 inhibitors. Combining PDE5 inhibitors with nitrates can cause a dangerous drop in blood pressure. If you take nitrates, you will need to use a different ED treatment.
Pay attention to side effects of your ED medication
Are there side effects? Yes, there can be. Some men get headaches or muscle aches when they take these drugs. Others get a stuffy nose, a flushed face, or indigestion. For most men, these effects are mild.
Men who take Viagra might notice temporary vision changes, where things look like they’re in a blue-green filter. If your visual acuity (how well you see) changes, you must stop taking the medication and inform your doctor immediately. Cialis users sometimes experience back pain.
If any side effects give you trouble, reach out to your doctor and ask whether another ED treatment is right for you.
Self-injections
The medical term for this approach is intracavernosal injection (ICI). The success rate for this method is about 85%, according to the American Urological Association (AUA). As with all medications, however, the response will depend on many different factors, including the severity of the condition and the medication dose.

If you take this route, you’ll use a tiny needle to inject a medication called alprostadil into the side of your penis. Sometimes, other medications are mixed with alprostadil, so you might hear terms like bimix or trimix, depending on what is used. Ask your physician about the differences between these medications and how they work.
After the injection, an erection usually starts within 15 minutes and can last up to two hours. Don’t be alarmed if your erection lasts a while after you ejaculate. That can happen.
However, if you have a rigid erection that lasts longer than 4 hours, head to your local emergency department. This condition is called priapism and you’ll want medical attention ASAP.
If you use ICI, make sure you space each injection at least 24 hours apart. Up to 3 injections a week should be safe but ask your doctor about the right plan for you. Using ICI too often can scar the penis, which can make erections more difficult later on.
The idea of giving yourself an injection in the penis might make you queasy, but lots of men manage their ED this way. Your doctor will teach you how to do it safely for effective results and minimal pain. Your partner can also be taught how to do it.
Urethral Suppositories (MUSE)
The drug alprostadil (also used in injections) can come in suppository form, too. With the MUSE intraurethral method, you place a pellet into your urethra – the tube that allows urine and semen to leave your body. An erection usually starts within 10 minutes, when the drug gets absorbed and moves from the urethra into the erection chambers, the corpora cavernosa. Typically, the erection lasts for 30 to 60 minutes.
As with self-injections, your doctor will show you how to use MUSE safely and effectively. Side effects may include pain in the penis, testicles, legs, and the area between the scrotum and rectum. Some men feel warmth or burning sensations in the urethra, and the penis might redden. There could be some minor bleeding, too, if you don’t place the pellet correctly.
Testosterone therapy
If your testosterone levels are lower than normal (below 300 ng/dL), your doctor might suggest testosterone replacement therapy (TRT).
Testosterone is an important hormone for men. It drives male-typical characteristics like a lower voice and body hair distribution. It also drives your libido.

But in some cases, men’s bodies don’t produce enough testosterone. Also, men’s testosterone levels naturally drop as they get older. It’s a normal part of aging.
Your doctor might start you on TRT if you have other symptoms of testosterone deficiency, like low sex drive, depressed mood, or fatigue. You’ll follow up with your doctor periodically to see how well it’s going.
Don’t get duped! You might find over-the-counter products that claim to contain testosterone to improve sexual performance. Lots of men think about trying these on their own, without seeing a doctor. But it’s essential for your doctor to measure your testosterone levels and monitor them over time. Your doctor may also want to conduct other important blood tests.
Testosterone should always be taken by prescription. Think about it. Do you really want to trust your sexual health to the convenience store on the corner or a shady website?
Vacuum erection devices (VEDs)
If you don’t do well with medications – or can’t take them – you might try a VED, a simple mechanical tool. As the name suggests, a VED triggers an erection by using a vacuum to bring blood to your penis.
The basic components of a VED are a plastic tube, a small hand pump, and a rubber O-ring. Here’s how they work together:
- When you’re ready to have an erection, you place your penis into the plastic tube, and hold it close to your body.
- Next, run the hand pump for about one to three minutes.
- Once your penis is fully erect, you place the O-ring around the base of your penis to keep the blood inside.
- From there, you can remove the tube and have intercourse.
- When you’re done, remove the O-ring.
VEDs have their pros and cons. On the pro side, they can be used at any VEDs have their pros and cons. On the pro side, they can be used at any time, so you can always be ready for sex. You don’t need to take any medication, and there’s no surgery involved. And if used properly, about 75% of men have success, according to the AUA. Your doctor will show you how to use it. Again, for any individual patient, the response depends on the severity of the condition and many other factors that your doctor can discuss with you.
On the con side, VEDs can be a little cumbersome. They take about 5 to 10 minutes to set up, which means you and your partner will have to take a short break during lovemaking so you can get an erection started. Some couples find this interruption less than romantic, and it might take away some of the excitement and spontaneity.
Other drawbacks to the VED: Your erection might look a bit floppy because there’s no erection/additional blood stored between the O-ring and your body. Some men find that their ejaculation feels different. You could feel some coldness or numbness in your penis, too.
Note: Sometimes, a man’s body shape makes it difficult to use a VED. Also, men who have problems with blood clotting and those who use blood thinners shouldn’t use VEDs.
Revascularization surgery
Younger men with ED caused by pelvic trauma may benefit from revascularization surgery. This process involves using an artery from the abdomen to create a “bypass” in the penis.
Revascularization is a very uncommon and specialized surgery that is ideal for young men, often trauma patients, who do not have general vascular disease since the “new” connection needs to be “atherosclerosis free” to be able to bring blood to the penis.

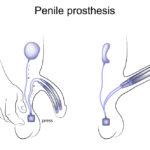
Penile implants (prostheses)
What, exactly, is an implant? It’s a device that’s surgically implanted into your penis and helps you create an erection on demand.
Implants come in two types:
- Malleable implants are semi-rigid bendable rods, usually made from silicone. When you want an erection, you simply move your penis into an upward position. When you’re finished with sex, you can move it back down.
- Inflatable implants are cylinders that fill with fluid to create an erection. You control the timing by using a special pump that is also surgically implanted, usually in your scrotum. You can start an erection with just the press of a button. After sex, you can push the same button to deflate the cylinders.
Getting an implant is a big decision. Once you have one, there’s no going back. That’s because the rods or cylinders replace two chambers in the penis called the corpora cavernosa. These are the chambers that normally fill with blood during an erection. During implant surgery, the corpora cavernosa are removed completely.
Implant surgery is fairly straightforward. Chances are, you’ll spend a night in the hospital, although you might go home the same day. You’ll probably have some pain, bruising, and swelling for a few weeks. Your doctor will give you special instructions about lifting things and exercising. You’ll need to wait about 8 weeks before having sex again.
Like any surgery, implants have risks. You might develop an infection. There’s also a slim chance that the device will malfunction, and you might need surgery again to fix the problem. However, most men with implants have successful, satisfying sex lives for many years after surgery.
Implants do have high satisfaction rates among men and their partners. In fact, some partners might not even know you have an implant. And orgasm should feel the same.
How about supplements?
Some men find it helpful to take supplements and herbs, but your mileage may vary. No matter what, always check in with your doctor before taking any product. Supplements aren’t regulated by the FDA the way drugs are, and you might not know how a product will interact with other health conditions or medications.