Kidney Cancer
Table of Contents
- Introduction to Kidney Cancer
- Causes and Risk Factors
- Symptoms
- Diagnosis
- Staging and Grading
- Treatment
- Post-Cancer Treatment
Introduction to Kidney Cancer
Cancer is a condition characterized by an uncontrolled division of abnormal cells, that often invade and distort the structure and function of surrounding normal tissues. There are two major types of kidney cancers on the basis of their origin.
- Primary Kidney Cancers: These cancers originate from the kidney cells.
- Metastatic Kidney Cancers: These originate from a distant site. Some of the cancerous cells land into kidneys through the bloodstream where they start their cancerous activity.
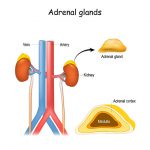
What are Kidneys?
Kidneys are two bean-shaped organs located against the posterior abdominal walls on both sides of the spinal cord. There are multiple functions of kidneys. They remove toxic substances, play a role in blood production, maintain blood pressure, and also have a part in the endocrine system. The kidneys produce a hormone called erythropoietin which induces red blood cell proliferation. The kidneys also have a central role in blood pressure management by the activation of the renin-angiotensin system. When blood passes through the kidney slowly, the kidney recognizes it as dropping blood pressure. It then activates certain enzymes that increase sodium reabsorption and thus, water also moves back into the body instead of going out in the urine. This increases the blood pressure. The excretory function of the kidney also is well-known as it removes all waste products from the body. The endocrine function of the kidney is to help in vitamin D production.
When the kidney is diseased, all these important mechanisms are impeded and ultimately the homeostasis of the body is disturbed.
Key Statistics Regarding Kidney Cancer:
The worldwide incidence of kidney cancer varies. In the United States, renal cell carcinoma (RCC) is the most common cancer in adults1. Globally, RCC is the ninth most common cancer in men and the 14th most common cancer in women. There were about 143000 deaths reported in 2012 due to RCC that makes it the 16th most common cause of death globally2. The probability of this increased prevalence of RCC all over the world is the frequent use of advanced imaging modalities. The CT scan is done commonly for the diagnosis of other diseases often picks up kidney cancer at a very early stage.1
Causes and Risk Factors
Cancers originate from mutated and abnormally fast proliferative cell groups. Cell division is a complex process. It involves not only the division of cell and its organelles but the genetic material in the form of DNA also has to be duplicated. During the duplication of DNA, certain genetic mistakes commonly occur. These mistakes are corrected by a special anti-cancer protective system present in the cell. However, some defected cells sometimes escape the checking process of the anti-cancer protective system. These cells then grow abnormally to give rise to cancer. The same mechanism occurs in kidney cancer. Thus, all kidney cancers arise because of a genetic defect in a cell. The genetic makeup of some individuals is such a way that allows easy cancer origination, which explains why certain people are known to have cancers running in their families, in other words, family history can be significant in the origination of cancer.
In addition, there are certain other factors that increase the risk of mutations in cells and subsequently cancers. These are:
- Male gender: Men are known to have increased risk of kidney cancers than women. 3
- Older age: The elderly population is prone to have a number of cancers. The genetic mutations tend to increase as a are part of senile changes. Kidney cancers are also more prevalent in old age. 3
- Hypertension: Hypertensive patients depend on life-long blood pressure-lowering antihypertensive therapy. The effects of both hypertension and antihypertensive therapy may induce carcinogenesis (initiation of cancer) in an individual.4
- Smoking: It is a risk factor for numerous cancers such as lung, esophagus, larynx, breast, kidney cancer, and more. The effect of carcinogens (substances that initiate and promote cancer growth) found in cigarettes is an important risk factor for kidney cancers. 4
- Industrial effects: Individuals working in industries, where there is increased exposure to asbestos, coal, pesticide, vinyl chloride, benzene, and copper sulfate, etc., have a substantially high risk of kidney cancers.4
- Radiation exposure: Patients who have been treated with radiations for other cancers such as cervical cancer are prone to develop kidney cancer. 4
- Hereditary factors: Genetic makeup of some individuals can make them more vulnerable to develop cancers of certain types. 4
- Lifestyle factors: Obesity is a major risk factor for the development of kidney cancer. This may be due to low levels of vitamin D in obese people, which is essential for inhibitory effects on cancer growth. The dietary factors include consumption of coffee, alcohol and other beverages. 4
Symptoms of Kidney Cancer
Kidney cancers have some specific symptoms that are related to kidney functions and some general symptoms that occur because of the rapidly growing mass in the body. The symptoms which occur as a part of general body response include:
- Weight loss: This is a sign of advanced disease. You may notice excessive sudden weight loss. The reasons for weight loss are decreased appetite, continuously dividing cancer cells that are consuming most of the nutrients of the body and, nausea and vomiting.
- Loss of appetite: You may notice that your appetite is decreasing. This is also a sign of advanced-stage cancer. It occurs because of the direct effects of cancer or psychological ill-being secondary to cancer.
- Extreme fatigue: When your appetite decreases and you start losing weight, your body responds to it by getting fatigued. You will notice that you get tired very easily.
The symptoms of kidney cancer related to structural distortion and functional disturbances of the kidney are:
- Blood in urine
- Constant pain in flanks (middle of the trunk, where kidneys are located)
- Presence of lump in the abdomen
- Anemia
There are certain other symptoms that occur when kidney cancer metastasizes (spreads) to distant organs. These are:
- Lungs – shortness of breath, cough, etc.
- Bones – extreme bone pain, easy fractures, etc.
- Brain – neurological issues, etc.
Diagnosis
The diagnosis of cancer is made by biopsyand histopathological confirmation of abnormal cells. 6 A biopsy is when a small piece of cancerous kidney tissue is taken and viewed under a microscope to differentiate healthy and cancer cells. There are some other tests that your doctor may order to look for kidney function, distant organ metastases, and to stage cancer.
Blood tests:
In these tests, your doctor checks the blood chemistry. The presence of anemia may indicate a declining kidney function.
Urinalysis:
In this test, your urine color, composition, and chemistry are evaluated. The significance of urinalysis in kidney cancer is it helps in determining the structural damage due to cancer. For example, the presence of blood in urine indicates an invasion of cancer into blood vessels distorting their anatomy and allowing blood leakage.
Liver function test:
This test is used by your doctor to see the metastases of cancer into the liver. Deranged liver function tests are predictive of liver metastases.
Imaging:
The imaging is very critical for the staging of cancer and to see the extent of metastases. 5 The following imaging test may be ordered by your doctor:
- Intravenous pyelogram: This is a special type of x-ray in which a contrast dye is injected in a vein. The dye moves through kidneys, ureters, and bladder while simultaneously X-ray photographs are taken. It helps in ruling out the presence of cancer in these organs.
- CT (Computed Tomography) scan: In this test, the X-ray machine takes pictures of various organs from different angles. All pictures are then assembled with the help of a computer into a single photograph. Sometimes a dye is used to improve the quality of the picture and see different organs clearly.
- MRI (Magnetic Resonance Imaging): In this test, rays from a magnetic field are used to take a photograph of the organs. This test helps your doctor to see more clearly what is going inside your body.
Biopsy:
This test is performed with the help of a needle that is inserted into the kidney. A camera is used to see the inside of the body and allow the needle to reach safely at the targeted site without damaging other organs. The needle may extract some cancerous tissue. This sample is then sent to a laboratory where slides are prepared. The histopathologist then confirms the presence of cancer by looking at the slides.
Grading and Staging of Kidney Cancer
Grading of the Cancer:
Grading of the cancer is done by looking at the nature of cancer. Low-grade cancers are those that have an indolent course. They grow slowly and do not have the potential to spread out. High-grade cancers are those that divide very rapidly, have aggressive behavior, and tend to spread locally. Grading is done numerically on a scale of 0 to 4.
- Grade X (0): The grade of this cancer is not known, which means cancerous activities may be going on at a molecular level.
- Grade 1: These are cancer cells that resemble normal cells a lot. Grade 1 cancers are low-grade cancers.
- Grade 2: These are cancer cells that are moderately different from normal cells. These cancers lie at the borderline of low-grade and high-grade cancers.
- Grade 3: These are cancer cells that are very different from normal cells. These are considered high-grade cancers.
- Grade 4: These are cancer cells that are completely different from normal cells. These are also high-grade cancers.
Staging of The Cancer:
Staging of the cancer is done on the basis of how far cancer has reached i.e. its confinement to kidney or involvement of surrounding tissues and lymph nodes and metastases to distant organs. The most commonly used method to stage cancer is the American Joint Committee in Cancer (AJCC). The staging of kidney cancer is done by the TNM method.
- T indicates the size of the primary tumor
- N indicates the involvement of nearby organs and lymph nodes
- M indicates metastasis to distant organ
Further, numbers are assigned to T, N, and M, and a combination of these tells the actual size and location of cancer and the involvement of surrounding tissue and metastasis.
The TNM classification of kidney cancer is: 7
T – Primary Tumor
- TX: Primary tumor cannot be appreciated
- T0: No evidence of primary tumor
- T1: Tumor is confined to the kidney and is equal to or less than 7 cm
- T1a: Tumor is equal to or less than 4 cm
- T1b: Tumor is 4-7 cm
- T2: Tumor is confined to the kidney and is >7cm
- T2a: Tumor is >7 cm but <10 cm
- T2b: Tumor is >10 cm
- T3: Tumor extends beyond the kidney to involve the major vessels and surrounding tissues till Gerota’s fascia (outer covering of kidney) BUT NOT adrenal gland
- T3a: Tumor extends BELOW the diaphragm
- T3b: Tumor extends ABOVE the diaphragm
- T4: Tumor has spread beyond the Gerota’s fascia
N – Regional Lymph Node Involvement
- NX: Regional lymph nodes cannot be assessed
- N0: No metastasis in regional lymph nodes
- N1: Metastasis in regional lymph nodes
M – Distant Metastasis
- MX: Distant metastasis cannot be assessed
- M0: No distant metastasis
- M1: Distant metastasis
For example, if your doctor says your stage is T2 N1 M0, it means that tumor size is limited to the kidney but locally it has spread to involve lymph nodes (N1); whereas, metastasis has not occurred yet (M0).
Treatment
The management of kidney cancer varies according to age, previous medical history, current medical issues, and the stage and grade of cancer. 8 Depending on these factors, your doctor may advise you the following treatment options.
Surveillance:
In this, no treatment is offered; rather close observation of tumor is done. The doctor advises this treatment when you have a benign tumor. Benign tumors are masses that look like cancer but grow very slowly and are not harmful. Other reasons for the recommendation of this treatment plan are the refusal of the patient to other options or the poor health status of the patient that does not allow a treatment.
Laparoscopic ablation of kidney cancer:
Laparoscopic procedures involve the use of highly specialized machinery that allows cancer to be destroyed within the body by the use of either extreme heat or cold. It involves minor surgical cuts and preserves the remaining healthy tissue.7
Surgery:
The surgery is the standard treatment for the removal of kidney cancer from the body especially for stages I, II, and III. 7 Depending on the grade and stage of cancer, the kidney is either partially or completely removed. The goal of the surgeon is to spare the healthy tissue as much as they can. When both kidneys have to be completely removed from the body, then the patient depends on dialysis for cleaning and purification for blood.
The operation that removes the kidney from the body is called nephrectomy. There are two types of nephrectomies:
- Radical nephrectomy: It means that the entire kidney is removed with its nearby organs (adrenal glands and lymph nodes).
- Partial nephrectomy: It means only the diseased portion of the kidney is removed.
These operations are done either by traditional open surgery method or more advanced options like laparoscopy. Laparoscopy is the use of machinery that allows the surgical instrument to enter the abdomen through small holes. Then, with the help of a camera, the surgeon performs surgery by looking (inside the abdomen) at the monitor.
Cytotoxic therapy:
In this treatment plan, your doctor prescribes certain drugs that directly kill the cancer cells by blocking proteins and new vessels formation that are providing essential nutrients for the growth of cancer cells. It is reserved for patients who have metastatic advanced disease. Options include
- Biological therapy/ immunotherapy: These drugs utilize the components of the body’s immune system to fight cancer.
- Chemotherapy: These are potentially toxic drugs that destroy cancer cells.
- Radiation therapy:
It involves high-energy radiations to mitigate the symptoms of metastatic and advanced-stage cancer. It is actually not a therapy to treat cancer; rather it is done to alleviate the symptoms of cancer.
Clinical trial:
Your doctor may offer you to enter a clinical trial program. These are researches done on a large scale to investigate new treatment options for different diseases and different individuals.
Post-Cancer Treatment
- After treatment, your doctor may advice follow-up care. Follow-up care includes close monitoring in case a recurrence occurs. It involves routinely testing of the kidney. These tests may be similar to those your doctor ordered for the diagnosis of kidney cancer. The duration of the follow-up depends on the type of cancer.
- You have to take some precautions yourself. It includes modification of your lifestyle. Some common and basic tips are:
- Smoking is associated with a high risk of recurrence in post-cancer-treated patients, so quit smoking. 9
- Cut down alcohol intake.
- Keep your dietary intake healthy.
- Do exercise and stay active.
- If you have a kidney removed after post-cancer treatment, you need to be more careful. Make sure to avoid:
- Major contact sport
- Self-medication (especially NSAID’s- nonsteroidal anti-inflammatory drugs)
- Excessive protein and salt intake
- It is essential to manage co-morbidities, such as hypertension, high cholesterol, diabetes, and obesity, for better and prolonged kidney functioning. 9
References:
- Chow, W. H., Dong, L. M., & Devesa, S. S. (2010). Epidemiology and risk factors for kidney cancer. Nature reviews. Urology, 7(5), 245–257.
- Znaor, A., Lortet-Tieulent, J., Laversanne, M., Jemal, A., & Bray, F. (2015). International variations and trends in renal cell carcinoma incidence and mortality. European urology, 67(3), 519–530.
- Ljungberg, B., Campbell, S. C., Choi, H. Y., Jacqmin, D., Lee, J. E., Weikert, S., & Kiemeney, L. A. (2011). The epidemiology of renal cell carcinoma. European urology, 60(4), 615–621.
- Pascual, D., & Borque, A. (2008). Epidemiology of kidney cancer. Advances in urology, 2008, 782381.
- Reznek R. H. (2004). CT/MRI in staging renal cell carcinoma. Cancer imaging : the official publication of the International Cancer Imaging Society, 4 Spec No A(Spec No A), S25–S32.
- Sahni, V. A., & Silverman, S. G. (2009). Biopsy of renal masses: when and why. Cancer imaging : the official publication of the International Cancer Imaging Society, 9(1), 44–55.
- Swami, U., Nussenzveig, R. H., Haaland, B., & Agarwal, N. (2019). Revisiting AJCC TNM staging for renal cell carcinoma: quest for improvement. Annals of translational medicine, 7(Suppl 1), S18.
- Campbell, S., Uzzo, R. G., Allaf, M. E., Bass, E. B., Cadeddu, J. A., Chang, A., Clark, P. E., Davis, B. J., Derweesh, I. H., Giambarresi, L., Gervais, D. A., Hu, S. L., Lane, B. R., Leibovich, B. C., & Pierorazio, P. M. (2017). Renal Mass and Localized Renal Cancer: AUA Guideline. The Journal of urology, 198(3), 520–529.
- Kim, H., Kim, M. H., Park, Y. S., Shin, J. Y., & Song, Y. M. (2015). Factors That Predict Persistent Smoking of Cancer Survivors. Journal of Korean medical science, 30(7), 853–859.